We tend to live our lives working on the edge in today’s world
…Some people enjoy it – “Adrenaline Junkies” and some dont (Me and believe most of us). Believe it or not …we are all becoming one of them (Adrenaline junkies I meant). Its either because of our bosses, wives, parents or peers (better to blame others). In reality its us…We are forgetting how to prioritise our lives.
Living a life where you are constantly on the go is exciting but takes its toll on our body and mind…..BTW speaking of mind…As ophthalmologists our entire world revolves in and around 24 mm of space of the eye ball. We are inclined (Voluntarily/Involuntarily) towards forgetting the rich knowledge imparted onto us during the golden years of our graduation. This period taught us a lot many things about the miracle of nature – The Human body and its “central processing unit” – The BRAIN.
Everyone seems to have one but it is seldomly used by most.
The anatomy of the human body and its understanding hasn’t really changed much in the last couple of centuries (Dua’s layer being an exception), however its physiology is a constant dynamic entity which is still being researched upon. We know what the BODY is, but we are still trying to understand how it works, how it functions.
Going back and in the process of trying to understand myself, I happened to stumble upon an entity which finds mention in allied disciplines such as Homeopathy and Ayurveda ( I can hear the groans from the idealistis) but is rarely mentioned in the medicine textbooks of allopathy. Sigmund was a dude…unfortunately people are still trying to understand what he said and what he didnt…
Anyways…..with the recent developments in the field of “Science” and the need to publish something (PUBLISH OR PERISH Click if you like), Psyhcologists/Psychiatrists/Shrinks have acknowledged the presence of this entity known as “SYMPATHETIC OVERACTIVITY” (Ta daaaaann).
I shall try to explain this physiological process which when thrown into an overdrive can have some really nasty (pardon me but by ‘nasty’ i meant SHITTY) adverse effects in a variety of ways.
With the ever so competitive world driving us towards the brink of insanity,
we are often compelled to throw our “Flight or Fight” response into play more than it is required. Wondering what do I actually mean? Let’s pay a visit back in time to the physiology class where we usually spent sleeping (Presuming you were like me and presumptions/assumptions are usually correct & even if they were not…who cares).
[Setting – 1st year MBBS, classroom, Not so sympathetic Physiology prof (sorry sir), talking in a monotonous voice (enough to put even the gods to sleep)]
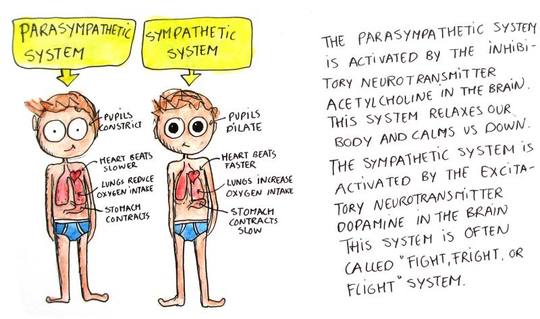
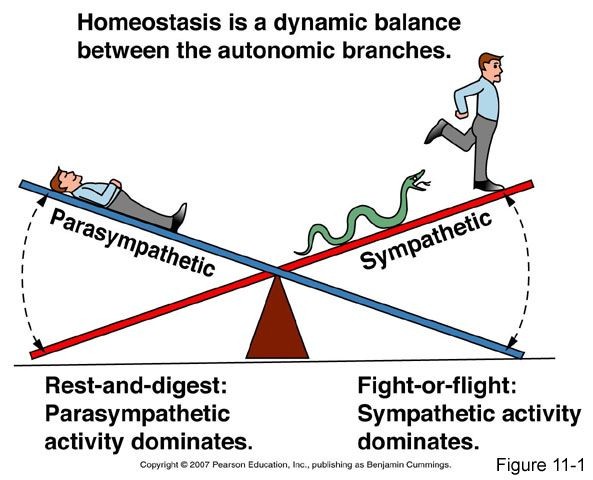
Definition of Sympathetic system: The sympathetic nervous system (SNS) is one of the two main divisions of the autonomic nervous system, the other being the parasympathetic nervous system. [Source] [Source]
The autonomic nervous system functions to regulate the body’s unconscious actions. The sympathetic nervous system’s primary process is to stimulate the body’s fight-or-flight response. It is, however, constantly active at a basic level to maintain homeostasis. [Source] The sympathetic nervous system is described as being complementary to the parasympathetic nervous system which stimulates the body to “feed and breed” and to (then) “rest-and-digest”.
The sympathetic nervous system is responsible for priming the body for action, particularly in situations threatening survival, [Source]. Sympathicotonia is a stimulated [Source] condition of the sympathetic nervous system, marked by vascular spasm, [Source] elevated blood pressure, [Source] and goose bumps. (ZZZzzzzzzzzzz)
Ok…wake up ….rise and shine…the lecture is over….You’ve got the definition.
So for me till date “Sympathetic system” was synonymous with “Sympathy”(something which we never got) and “Parasympathetic system” was its kryptonite. Apparently Sympathetic system plays a huge role in our day to day lives. Right from operating in the OT to driving, from playing on the mobile to paying a visit to the loo (Loosens up the sphincters as well).
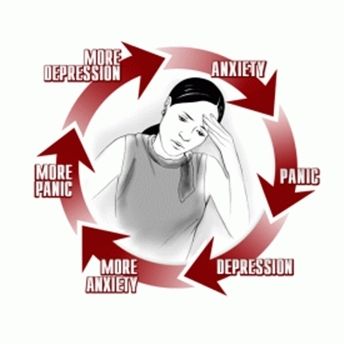
Thrown in to over drive – ‘ANXIETY’ is the collection of symptoms caused due to Sympathetic activity overdrive and STRESS is what precipitates it. When overdrive is in the top most gear the resultant condition is a “Panic attack”. Anxiety is a phenomenon which is very much subjective. In fact the old saying “Still waters run deep” holds true for most of the medicos.
“THOU SHALL NOT REST”
When examining the patients we are constantly on the vigilance (Are the relatives going to hit me??). On one hand we are trying to do justice to the patient and on the other hand we are trying to be legally, diplomatically, NDTVically, Congresstically, BJPtically, Arnab Goswamitically and financially correct.
The medical professionals are required to maintain a “Poker face”
when facing the patients and the relatives, when there is a great deal of turmoil inside (not the turmoil of bladder). We often ourselves mistake this for “being in control” when we have succeeeded in maintaining an emotionless face.
In reality what is the result is, a DEEP & HEAVY IMPACT on our autonomic system which is made to run continuously never taking a break.The susceptibility to chronic stress varies among individuals and changes across lifespan. Working in a corporate or under someone, achieving targets or examining maximum number for patients for the sake of surgeries, STRESS is usually the ultimate result. The stress puts our body to activate the sympathetic system.
Operating 100s of cases in day, seeing 200s patients in the opd. Have to finish the OPD but yet do justice to the patient. Finish OPD and move over to the ot. Finish OT and move over to the OPD. The OPD sister is un-coperative, the patient is un-coperative, the seniors are un-coperative, the consultants are un-coperative. Blah Blah Blah…..STRESS STRESS STRESS.
Living on “Stimulants” such as coffee, energy drinks (Tapri ki Chai included) and combined with the stress of the profession, we agitate our bodies to a point where we are unable to calm down.
So basically speaking in normal terms… we are brewing up a storm within ourselves which becomes self sustainable and self propagating. Its like the Juggernaut…Not stopping (Even for a pee). Round the clock stress just puts the sympathetic system in the “Autopilot” mode which is active even during our sleep.
Sleep deprivation and fleeting attention from one stressful situation to another, we are plagued by the stress of striving for perfection. We tend to perform the same task 20 times: ten times in our head before the actual event, once during the event and nine times after the event as we analyze how we could have improved our performance.
Combined with the other factors the need to be omnipresent on the social media (Oh yeah
– “SELFITIS” is an “IN” thing) , the conferences, the news and the academic front just adds to the trouble. The constant desire to prove ourselves to others and achieve celeb status ( I did it – I created someting new and F@#$ myself) is just adding to the troubles.
Waise going back to social media….Taking and posting Selfie has been officially been declared a mental disease. Come to think of it…why do we take selfies???
Because Its the only way we are seeing ourselves smiling…looking into the mirror in the morning we are too busy thinKing of the day ahead and what we are gonna face (Indian doctors leave the house with the ‘KAFAN’ tied around their head). So back to the topic….posting the selfies as soon as they are taken on the social media just to prove who all you’ve been with (Im a culprit too…but hey!..its what everybody does) in the conference so that u can increase the footage is another thing that stimulates the Sympathetic system. You shall not be able to rest till the point you post it.
“THOU SHALL NOT KNOW HAPPINESS”
Ever wondered why some of us dont feel happy after coming back home and would want to spend few moments more in the hospital/clinic/chamber/car to finish that study/project/social media post?? Ever wondered why the only thing buzzing in your mind is the damn INTERESTING CASE you saw in the morning even when your head hits the pillow?? Ever wondered why your colleague (opposite gender or in some cases same gender ;) suddenly seems more interesting than the family??…why the extra marital affairs are on the rise?? Is something such as workplace husband or wife normal?…Read below
Sympathetic system also helps us in achieving our goals by providing the driving force. This ensures the reward center being constantly stimulated which ultimately programmes our mind to associate the activity which stimulates the sympathetic system with pleasure and rewards. Most often THIS is our professional life and that’s where we get inclined leading to marital problems.
Your spouse if not from the same field suffers the most.
Your colleague (Again .. opposite gender or in some cases same gender ;) is something which is treated by ur subconcious/unconcious mind as a part of that “ACTIVITY” which shall reward you and satisfy the satiety of your reward center. Try spending some quality time with your family and suddenly your WIFE/HUSBAND again becomes attractive(ROFL).
The inability to concentrate on activities at home
(Like peeing in the basin or venturing out of the washroom without your shorts) after a long day of work at the professional front indicate the wearing off the sympathetic system activity. This often forces many of us to choose between the two, the professional or the domestic life. Striking a balance becomes difficult for many of us.
You need references and citations for eveything. Everything needs to be justified and clarified. I remember asking my mechanic the references and studies when he mentioned that the new engine oil will give me better mileage.
“THY BODY SHALL PERISH!”
Insomnia, acid reflux, headaches from jaw clenching, increased muscle tension leading to cramps and chronic muscular pain, constipation, frequent urination, low libido, palpitations, hypotension/hypertension, adrenal fatigue, poor digestion, cold extremities, restless legs, urge to keep on walking, compromised immunity are few of the symptoms to name. The need to continuously chew on the gum is also a way of trying to vent out the stress.
Basically u r on the verge all the time. The moment someone utters something which might not be justified….you want to lash out and kill the poor person, Strangle him, bang his head on the wall (Not me…I am cool as ICE 🙂)…
Lack of energy, lack of joy, SELECTIVE decreased LIBIDO, decreased ability to handle stress, a compromised immune system and memory lapses which all eventually lead to a sub clinical depression where the only stimulant for the mind is the activity associated with the activation of the sympathetic system (AGAIN AGAIN …. opposite gender or in some cases same gender, Social media, PUBLICATIONS, STUDY, PROJECT…..)This gives us a false sense of happiness (In pursuit of happyness).
Oh yeah!“Rushing women syndrome” is another term coined by few which is applicable to men as well.
“Thou shall Know!”
Parasympathetic system activation is the key. It’s the “Rest and Digest” system of our body.
Remember you are not “SUPERMAN/WOMAN”. You need rest. You need to be happy. You deserve to be happy. Get your priorities right and understand that you need to get back your life. The need to succeed should not be a burden or a curse or a punishment for your family. The constant need to prove oneself should be stopped. The cycle needs to be broken. Any habit to be formed takes 20-30 days. Hence that is the period where you shall have to pay attention and avoid the above mentioned urges. Once it becomes a habit, you shall find bliss. Then slowly steadily reintroduce your priorities one by one.
Think and decide, DO I NEED TO FINISH THE OPD? DO I NEED TO OPERATE SO MANY PATIENTS IN A DAY? DO I NEED TO TOLERATE THE OPD SISTER?…PRIORtise your life. Safely eliminate the “STRESSES” of your life.
We forget to prioritise our life and activities and hence feel overloaded with work (like my desire right now to complete this damn blog and publish it).
Sleep is critical in order for the body to heal and repair. Break away from the electronics and unplug from the digital world for a few hours every week. Yogic exercises are a great away to achieve this. Try following Modiji for a change…:).
However realization and acceptance shall be the first step. Managing and maintaining ‘Mindfulness’ round the clock is the key. Once that is achieved the next step is the activation of the parasympathetic system to help us in analyzing the situations and coming to conclusions. Mindfullness is the key to success. Thats what the stalwarts do.
One way is delayed reaction(except in the OT). Whenever a situation arises, think about it and forget it. Try not reacting immediately. Sleep over it and give it sometime. Somehow it shall seem trivial later and the answers shall come easily.
Wouldn’t it be ironic if I suggest the use of GOOGLE to find out the ways you can achieve the calm state by the balance of the autonomic system?
Diclaimer* – This blog is intended to bring forth the knowledge of how manipulative the world of research is. To avoid any complications and conflict of interest i shall make a deliberate attempt at not pointing out fingers towards any one or any journal conciously. Also the links are the most important part…everything else is garbage…so do click on them to get the real picture
.
Holub’s criticism: “especially where a scientist publishes has become much more important than what he is publishing” (Holub et al., 1991).
Recently i met a guy straight out of the Post graduation, done a decent number of surgeries & having a good knowledge of the subject. His only regret was that he wasn’t able to publish anything. The thought of not being able to publish anything was putting him down. He was losing his self confidence when other candidates having publications were preferred over him.
The motto “PUBLISH OR PERISH” had crept onto him and was sinking its teeth into his poor soul….for him essentialy his career was over…cause you see…he didnt publish anything, so all that was left for him was to “PERISH”.
We have all gone through that phase once in our careers where the pressure to publish has been tremendous. Just seeing your name up there in the “AUTHORS” list gives you a high which even an entire bottle of “Spirytus Rektyfikowany” cannot manage…
All this hype really bothers and makes me wonder…How does publication really help ???
So here I went ahead and did a little snooping around..talked to a couple of seniors and residents, approached the most faithful and loyal friend of the doctor, “GOOGLE” and joined a small distance based correspondence course in BIO – STATS just to understand what it really means…Some really interesting things came up…
The drive to publish or perish originated somewhere in the far west..obviously the brain child of some capitalist. The publication houses earn a ton of money and obviously dont really care about the common reader.
Its not only limited to Ophthalmology. The roots of this practice have spread in all specialities of medicine.
In simple terms….your article gets selected in a major journal (After you have become a grandfather), you pay the journal to publish it and then the journal gets paid for others to read.
So its a win win situation for the houses. In this process an old timer who has tons of experience but fails to put it on paper suffers and indirectly the readers are deprived of the golden knowledge. So you have “PAY TO PUBLISH & PAY TO READ“. This is a multi billion dollar market and the people in the country of the BIG SAM knew how to make profit out of it.
So came the open access journals with the “PEER REVIEW“..where only “pay to publish” was the motto. To counteract the “Predatory publishing“, peer review came to the rescue…I shall discuss this topic paticularly in detail later on.
Open Access is broadly split into two categories: Green and Gold.
Gold open access refers to the publishers making articles available to the public either entirely, or in part. This can take several forms itself, from being direct, delayed or a combination of both.
Direct open access accounts for around two thirds of all gold open access, and means that the publishers make the entire journal open access to readers with no limitations. The alternative, delayed open access, is when the most recent work is kept behind a paywall to subscribers but over time the articles are made publicly available for free.
Around a quarter of gold open access is the combination of both forms, known as hybrid open access, where the author or institution pays for the paper to be made public in what is traditionally a subscription-based journal.
Green open access is when an author makes the research available through self-archiving, and can take the form of pre-published manuscript or a published paper. PubMed Central is one example of this type of archive. (RUBY PROSSER SCULLY)
Since we are at the topic of pubmed…some facts..Pubmed on an average has 1.4 million to
2 million articles every year, half of which are never quoted again – Dr Stephen Leeder, emeritus professor of public health and community medicine at the University of Sydney.
They are forgotten like the forgotten memories of “INSIDE OUT” movie.
The rest are subjected to self citations and what not…also discussed later. Before you form opinions…let me clarify…there are some really good articles too, which deserve attention.
If you want something to be successful, just associate it with class superiority. Mercedes, Apple and many other such giants operated on this funda. The publication houses took a clue and went ahead with the same idea. Introduced the “BUG” of superiority in terms of the number of publications.
‘Oh yes we’re very proud of him. He’s in publishing you know!’
Higgs boson said that he probably wouldn’t have a job in today’s environment because he would not be considered “productive” enough. He has produced less than 10 articles uptill now…but takes pride in them.
Another factor which came into being is the funding.
Professor Virginia Barbour, chair of the Committee on Publication Ethics (COPE) earlier said that “Actually underlying this [is a] much bigger thing, which is this pressure to publish, We know that researchers experience this pressure to publish and this does actually lead them to cut corners [which] can lead to papers that may not be reproducible again down the line, It’s driven essentially by an obsession for how institutions are ranked, They are very dependent on the ranking of journals because funding flows to institutions in terms of how they rank. If you only reward people for one thing, that’s what they’ll work toward.” [INSPIRATION] [INSPIRATION]
Researchers are many, and competition for funding and employment is fierce in academic institutions. So how does an employer or funding body judge the achievements of a researcher?
One simple metric is the “Number” of research papers to their name. [SOURCE]
An infamous example was reported on the Australian funding system, where the system was reformed so that research money is now awarded based on publication count, and academics started to produce more papers but of lower quality (Butler, 2003).
So what started in the west for money..came to the east and the rest of the world as the Number game. People are just running after numbers not knowing the goal. The only goal achieved here in the east is “FAME“. The western counterparts earn money and the eastern counterparts earn Fame. Whatever is published there (in west i mean) is science and native journals are crap. So we are all running in the rat race to publish in the western journals.
Well fame is fame………
‘I haven’t been in any academic journals but I do get my Tweets re-Tweeted a lot.’
However you get it….which again brings me to something i feel many of you might relate to…or not…:D
There are four types of ophthalmologists..
First – They know their stuff….they know how to diagnose, operate and take care of patients. They,ve got the knowledge but unable to replicate on the paper. Some of these people are damn good clinicians and surgeons, but due to inability to “PUBLISH” or “ADVERTISE (how i see it)”, remain unknown to the majority of the opthalmological community. Though their patients are really happy and are well known in the community.
Second– They know how to diagnose, operate, take care of patients and also know how to put their results on the paper. These are the kind of people who inspite of being mediocre clinicians and surgeons (in some cases really exceptional clinicians and surgeons) attain the highest of positions and honors. Some of them are really gifted and can reproduce what they are doing on paper for the world to know.
Third – They may or may not know their stuff but have got really good sense of “BORROWING“ data and publishing it. They are usually co-authors in a number of studies though they dont have anything to do with the actual thing. They may be good clinicians or surgeons, but the lack of reproducing the data on paper is compensated by being a part of other’s.
Fourth – They are the ones who dont have good knowledge or publishing capacity and are just scrapping through. They train themselves in doing the most basic of things in ophthalmolgy and keep on surviving in this competitive world.
So how does it really matter to a young and budding opthalmologist???
Publication – Fame
Publication – Guide’s pet
Publication – Fame
Publication – More surgeries
Publication – Fame
Publication – Recognization as a competent doctor and surgeon (Even though thickness of posterior capsule is not known)
No Publication – No surgeries, ignored, no lasers, ignored, no fellowship, IGNORED conferences (R U KIDDING ME!!)…
Publish or Perish: ‘Welcome to the Team. Remember, if you follow the University Motto, you’ll do fine…’
The resident or fellow is not judged by his ability to save a sinking lens …..rather than the number of publications he/she has. Sad state. A resident spends more amount of time in trying to gather as many topics to publish than spending time in increasing his/her knowledge about the subject. Not all are gifted with the calibre to write….and not all gifted with the calibre to operate….Put Sachin Tendulkar in the kitchen and you will have a disaster. Intelligence quotient is relative.
The Clinicians can learn from Academicians and vice versa.Research is meant to be a noble and rewarding process.
The Movie “STUDENT OF THE YEAR” makes perfect sense. The competition is introduced to single out the best, rather it divides everyone and creates enimity, jealousy, low self esteem, aggression and finally resignation.
Forgot one thing, “PUBLICATIONS FOR PROMOTIONS“….the need to have specific number of publications for promotion in the teaching line is just ridiculous…A good teacher might not be a good researcher….and vice versa…but unfortunately the propaganda has been too strong..This often lead to the seniors hijacking the topics of the residents or setting up deadly deals with the residents (NO TOPIC, NO HOLIDAYS).
Before the “LIBERALS” defend themselves by saying that the academics is important for development and progress….go through the stats and explanations below.
This is how it progresses….
A study unrelated to the field of Ophthalmology but yet echoing a lot of other studies has raised eyebrows and doubts. I am giving the result of the study here.
“Tijdink JK, Schipper K, Bouter LM, et al
How do scientists perceive the current publication culture? A qualitative focus group interview study among Dutch biomedical researchers
BMJ Open 2016;6:e008681. doi: 10.1136/bmjopen-2015-008681“
ResultsFrequently perceived detrimental effects of contemporary publication culture were the strong focus on citation measures (like the Journal Impact Factor and the H-index), gift and ghost authorships and the order of authors, the peer review process, competition, the funding system and publication bias. These themes were generally associated with detrimental and undesirable effects on publication practices and on the validity of reported results. Furthermore, senior scientists tended to display a more cynical perception of the publication culture than their junior colleagues. However, even among the PhD students and the postdoctoral fellows, the sentiment was quite negative. Positive perceptions of specific features of contemporary scientific and publication culture were rare.
Conclusions Our findings suggest that the current publication culture leads to negative sentiments, counterproductive stress levels and, most importantly, to questionable research practices among junior and senior biomedical scientists.
Things you need to know before you jump into this quicksand.
Peer review – The gold standard???
Salami science, Euphemism
Self plagiarism
Gratitious helping.
Journal fever, Pathological publishing
Impact factor (actually i will be discussing this the last)
Self citations
Retraction watch
Manipulations.
Of course the medical hierarchy and hijacking.
Peer review (Referee system)!!!
So when i started as a resident …the first thing that was told to me was that “PEER REVIEW JOURNALS IS WHERE I SHOULD AIM AT PUBLISHING, CAUSE THEY ARE ‘FOOL’ – PROOF” …so tried my hand with a couple of them and everything got rejected…naturally got angry and kicked the “RESEARCH” papers under the bed and concentrated on becoming a surgeon rather than a journalist…
But with the recent increased interest in the Peer review journals and the number of publications i thought, why not find out more about the process and then apply…probably my papers would be accepted….here is what i found out…
‘A large Federal study published in the New England Journal of Medicine found that large federal studies don’t prove anything.’
Origin – Most often authors date the advent of what we now call editorial peer review to the 1752 Royal Society of London’s development of a “Committee on Papers” to oversee the review of text for publication in the journal Philosophical Transactions. Others insist the Royal Society of Edinburgh had a similar system in place as early as 1731. Peer review predates the invention of the scholarly journal. Early scientists circulated letters among their peers or read papers in society meetings to report the results of their investigations in hopes of response. Initially peer review was designed to assist editors in selection of manuscripts, rather than to authenticate findings, and the responsibility for integrity relied on the author. The origin of the process is from state censorship as developed through practices of state supported academies, as well as an attempt to augment the authority of a journal’s editor. It was not until the middle of the 20th century that medical journals used outside reviewers to vet manuscripts. (Fitzpatrick)
Please go through the below link to try and understand….something having its foundations on masala mix and manipulations cannot really sustain for long as the gold standard….
SO you know the origin, now lets understand the procedure…you submit a paper…the paper goes through the journal editorial board (usually a computer)…they send it out to scientists (working and hard working personnels themselves!!) …these guys read the whole thing (Guessing that they read, there are softwares to generate reviews)…understand/misunderstand/not understand/confuse the concept and then the review is given which is directed back to you. Now either you are rejected immediately or after making a number of corrections/alterations. This process can be blinded or not…What I mean is that the journal can select which persons should recieve your article or you can select on your own.
Do you understand??? so if you select yours …you can simply call up those people and can tell them..”PLEASE SELECT MY ARTICLE”..or just your name might be enough. As for the blind procedure…there are ways of getting around it too….take a look at this [SURPRISE].
“The Lancet editor Richard Horton has called the process “unjust, unaccountable … often insulting, usually ignorant, occasionally foolish, and frequently wrong.” Not to mention that identifying peer reviewers and getting their comments slows down the progress of science — papers can be held up for months or years — and costs society a lot of money. Scientists and professors, after all, need to take time away from their research to edit, unpaid, the work of others.
Richard Smith, the former editor of the BMJ, summed up: “We have little or no evidence that peer review ‘works,’ but we have lots of evidence of its downside.” Another former editor of the Lancet, Robbie Fox,used to joke that his journal “had a system of throwing a pile of papers down the stairs and publishing those that reached the bottom.” Not exactly reassuring comments from the editors of the world’s leading medical journals.
The two researchers, Douglas Peters and Stephen Ceci, wanted to test how reliable and unbiased this process actually is. To do this, they selected 12 papers that had been published about two to three years earlier in extremely selective American psychology journals.
The researchers then altered the names and university affiliations on the journal manuscripts and resubmitted the papers to the same journal. In theory, these papers should have been high quality — they’d already made it into these prestigious publications. If the process worked well, the studies that were published the first time would be approved for publication again the second time around.
What Peters and Ceci found was surprising. Nearly 90 percent of the peer reviewers who looked at the resubmitted articles recommended against publication this time. In many cases, they said the articles had “serious methodological flaws.”[SOURCE] [ORIGINAL ARTICLE]
Do you see the problem?? The papers are written by humans and assessed by humans…These reviewers are supposed to be “GATEKEEPERS” for the protection of the science, but most of them are practicing doctors and researchers…they have their own methods, interests, conflicts, pressures. A study submitted to a reviewer who might be working on a similar project will force the person to reject it. A single person serving on the review board of 20 journals, receiving 150 articles in a month, operating and attending to his patients is bound to make a mistake or miss something.
“The reasons it fails are similar to the reasons any human process falls down. Usually, it’s only a
“Cloning is all very well in theory, but do you have any proof it can actually work?”
few reviewers who look at an article. Those reviewers aren’t paid for their time, but they participate out of a belief in the scientific process and to contribute to their respective fields. Maybe they’re rushed when reading a manuscript. Maybe they’re poorly matched to the study and unqualified to pick it apart. Maybe they have a bias against the writer or institution behind the paper“.[SOURCE]
Authors sometime just jumble everything with a lot of figures and charts and make it difficult for the reviewer to understand. The reviewer just passes the paper and it ends up in the journal with absolute no relevance to the clinical science. Sometimes these papers do make an impact indirectly.
“In March 2015, BioMed Central (BMC) retracted 43 papers after it emerged that reviews had been fabricated across at least 13 different journals.
This scam, like several others that had come before, involved a form of self peer review where fake email addresses were provided to the journals for potential referees, but were ultimately used by the author themselves or their friends to write the positive review.
The BMC editors became suspicious after noticing misspelled names and mismatched email addresses.
An investigation revealed that the fraud appeared to be orchestrated by a third party company enlisted by the researchers to help with language and improving the reports.
The papers were retracted “because the peer-review process was inappropriately influenced and compromised,” the journal websites said. “As a result, the scientific integrity of the article cannot be guaranteed.”
Another example of flawed peer review was the publication of a widely-criticised study by NASA scientists claiming to show that arsenic had replaced phosphorus in the DNA of bacterium“. [SOURCE]
There is this following article which actually made a lot of sense and i am attaching the source of the article in the end.
“My coauthors and I wanted to know the impact such competition could have on peer review. We decided to conduct a behavioral experiment.
We invited 144 participants to the laboratory and asked them to play the “Art Exhibition Game,” a simplified version of the scientific publication system, translated into an artistic context.
Instead of writing scientific articles, participants would draw images via a special computer interface. And instead of choosing a journal for publication, they would choose one of the available exhibitions for display.
The decision whether an image was good enough for a display would then be taken following the rule of “double-blind peer review,” meaning that reviewers were anonymous to the authors and vice versa. This is the same procedure adopted by the majority of academic journals.
Images that received high review scores were to be displayed in the exhibition of choice. They would also generate a monetary reward for the author.
This experiment allowed us to track for the first time the behavior of both reviewers and creators at the same time in a creative task. The study produced novel insights on the coevolution of the two roles and how they reacted to increases in the level of competition, which we manipulated experimentally.
In one condition, all the images displayed generated a fixed monetary reward. In another condition—the “competitive condition”—the reward for a display would be divided among all the successful authors.
This situation was designed to resemble the surge in competition for tenure tracks, funding and attention that science has been experiencing in the last 15-20 years.
We wanted to investigate three fundamental aspects of competition: 1) Does competition promote or reduce innovation? 2) Does competition reduce or improve the fairness of the reviews? 3) Does competition improve or hamper the ability of reviewers to identify valuable contributions?
Here is what we found
Our results showed that competition acted as a double-edged sword on peer review. On the one side, it increased the diversity and the innovativeness of the images over time. But, on the other side, competition sharpened the conflict of interest between reviewers and creators.
Our experiment was set up in a such a way that in each round of the experiment a reviewer would review three images on a scale from 0 to 10 (self-review was not allowed). So, if the reviewer and the (reviewed) author chose the same exhibition, they would be in direct competition.
We found that a consistent number of reviewers, aware of this competition, purposely downgraded the review score of the competitor to gain a personal advantage. In turn, this behavior led to a lower level of agreement between reviewers.
Finally, we also asked a sample of 620 external evaluators recruited from Amazon Mechanical Turk to rate the images independently.
We found out that competition did not improve the average level of creativity of the images. In fact, with competition many more works of good quality got rejected, whereas in the noncompetitive condition more works of lower quality got accepted.
This highlights the trade-off in the current publication system as well.” [SOURCE].
I remember one of my seniors who had submitted an article got a reply back..”IT DOESN’T PROVE ANYTHING”…what the hell…this guy had a finding which nobody had noticed before…so with whatever resources he had, a submission was made…but unfortunaltely not accepted….3 years down the line i find people studying the same sign with great interest. SAD!!!
The crab mentality gets a gateway to impinge onto the pure world of science…
Self citations, Gratitious helping.
It basically means that you cite your ownself and others close to you….who inturn return the favour and the cycle continues…so you increase your own citations and indirectly increase the citations of the journal, boosting the impact factor…and hence the impact of your own article.
So its a game that is being played to glorify your ownself and others around you.
If you do it alone, its self -citation. Do it in a group and its “CITATION CARTEL or CITATION STACKING”. So there is an organized crime….take a look…[Banned Journals]. The Term Gratitious helping also comes in here. “You scratch my back, ill scratch yours”..A particular researcher quotes a study which is remotely concerned with his own and same is done by the person on the other end…The number of publications by a particular author (actually co – author) keeps in increasing till he reaches half century…then he is in the big league with everyone…really sad!!!
Now combine this “self – citation” with “salami science”, “manipulations”, “citation cartel” (love the word cartel – sounds so “GODFATHERISH”), “predatory publishing”, “self plagiarism and pathological publishing”…
There are ways to tackle this problem but ill leave that for later..
Now there are 2 school of thoughts….
First…if its your own work…you may do it…and if u r working in a team then you may do it…Second is dont do it at all….i would go with the second…see…if its your work…better complete it and then publish…why do you have to “SALAMI SCIENCE” it and publish…
It has been frowned upon in the “intellectual committee” and may have serious implications if discovered. …here is an example with its reference link below.
“Fowler and Aksnes (2007) did another research on the Norwegian database, but this time it was author rather than publication oriented. The percentage of author self-citation was rather low – 11% – but every self-citation yield, on average, 3.65 citations from others in 10 years. Fowler and Aksnes concluded that “self-citation advertises not only the article in question, but the authors in question.” In practical terms, this could mean that the author who managed to fit in even one more self-citation per article will be much better off years down the road than her colleague who didn’t. The effect turns negative only in very high levels of self-citations (40-50 a year). It seems that self-citation make authors more visible. It’s like with SAT preparation courses: it’s not that you’ll do better than the others if you take them; it’s that you’ll do worse than the others if you don’t take them. Because of this effect, Fowler and Aksnes suggest not only to remove self-citations from citation counts, but to penalize them as well. However, this could hurt older or more productive scientists, who cite more simply because they have more articles to cite and more publications where to cite them. Currently, every popular index has a version free of self-citations, but it seems that most people continue to factor them in.
But really, excessive self-citation is for amateurs: the real thing is forming a “citation cartel” as Phil David from The Scholarly Kitchen puts it. Phil Davis has done some detective work using the JCR data and found that several journals published reviews citing an unusually high number of articles fitting the JIF window from other journals. In one case, the Medical Science Monitor published a 2010 review citing 490 articles, 445 of them were published in 2008-09 in the journal Cell Transplantation (44 of the other 45 were for articles from Medical Science Journal published in 2008-09 as well). Three of the authors were Cell Transplantation editors. This is even nastier than excessive journal self-citation because, as Davis points out, self-citing can be detected without too much effort, but citation cartels are trickier. In the good news,three out of the four journals Davis reported as suspects of cartel behavior were suspended from the JCR, and Retraction Watch reports that two of the manipulating articles have been retracted“. [SOURCE]
Also the rising number of “MIS – CITATIONS” is another growing concern…”Researchers”have gone one step ahead and have started creating fictional and imaginary sources to claim the authenticity of their paper. [SOURCE]
Some useful links…where you might also find the ways to tackle it..
Salami publication or segmented publication is a distinct form of redundant publication which is usually characterized by similarity of hypothesis, methodology or results but not text similarity. These aspects of publications are not objectively detected by software applications and therefore present a serious threat to publication ethics
.
To tell it in lay man’s terms (like me) – Salami publication can be roughly defined as a publication of two or more articles derived from a single study (t2). Articles of such type report on data collected from a single study split into several segments just large enough to gain reasonable results and conclusions, also known as “Least publishable unit (LPU) or minimal publishable unit (MPU) or Euphemism”
From the publication ethics point of view, it is worse because it cannot be easily detected, gives undeserved credit to authors, misleads the scientific community and directly influences clinical practice by distorting medical evidence.
Example – Several groups of researchers took part in registered clinical trial on acute pancreatitis patients. The trial was designed as a longitudinal multidisciplinary study that observed diagnostic and clinical outcomes. Two groups of authors involved in this trial published two articles. One article described the prognostic value of interleukin 6 on late complication development in patients with acute pancreatitis in comparison to healthy controls. The other article presented the beneficial effect of enteral nutrition in patients with acute pancreatitis. The studied population was the same but the hypotheses of both articles were completely different and with different outcomes. Should those articles be published? Read in detail here..
There are many “RESEARCHERS” doing this to promote their numbers….and obviously with already a large number of studies to their credit they shall be able to get the successive ones published as well.
Predatory journalism
Conciously i am avoiding the predatory journals in Ophthalmology (many “AUTHORS” wouldnt be happy with their work getting discredited), the list to which you can find out quite easily on the net.
Ok…so the current journals work on “pay to publish” funda..so if you have a decent computer and know how to make a standard PDF which is available online to the people….CONGRATULATIONS!!! you can have your own journal…THE ADVANTAGES YOU ASK ME??? well…you can publish whatever you want and with whomever you may want..Have you ever gotten an email where you are asked to be an editor or preside over an editorial session or publish your work??? if YES…BINGO!!! Welcome to the world of predatory journalism.
A PubMed search was carried out to extract articles related to eye diseases during the period 2010–2014. Data was downloaded and processed for further analysis. A total of 62,123 articles were retrieved. A total of 3,368 different journals were found, and 19 journals were identified as “core journals” according to Braford’s law. And this was 3 years back …:O…Now now …i am not saying that PUBMED quotes the predatory journals…I am just trying to point out just how many articles are available out there..lol…
An analysis published in medical journal BMC Medicine found that the number of articles published in predatory journals jumped from 53,000 in 2010 to around 420,000 in 2014. (Avoiding Ophthalmology again).
Many of these articles will be published with lacking data..irrelevant analysis but concrete conclusions….and once into publication..these articles will then be modified (SALAMI SCIENCE to the rescue)…and published in other “BETTER” peer reviewed journals quoting the earlier articles. So you start small and then aim for the sky.
We have many such researchers working on and publishing in such journals and then moving onto the bigger ones…what they finally have is a long list of publications and impressive CV.
“It doesn’t mean that if you’re published in the New England Journal it’s automatically a wonderful paper, in fact there’s quite a lot of evidence that papers published in the big journals are more likely in the longer run to turn out to be wrong, because they’re kind of new and exciting (Rings any bells??) “. The main reason that journals persist is that they are the primary way that academics are assessed, yet the idea that what is published in the big journals is more significant or more likely to be right “is just plain wrong”, Professor Smith argues…whos he??? well he was BMJ’s editor of 25 years, Professor Richard Smith.
Over 50 per cent of publications in predatory journals come from researchers affiliated to private/government colleges within India, says a study which also sheds light on the contribution of national institutes to such poor quality open access (OA) junk journals. The assessment highlights the “publication pressure” among researchers and the “lack of monitoring of the research being conducted” as the major factors contributing to articles published in poor-quality predatory open access journals from India.
What is plagiarism? It is the noun of the verb “to plagiarize”. Webster’s dictionary describes it as ” to take without referencing from someone else’s writing or speech; of intellectual property”(precisely what i have done now …:D)…In lay man’s term – copy and paste,…now if u do it from someone else’s …its plagiarism and if you do it from your own its self plagiarism.
Its a very broad term and can actually be misread and misused….basically speaking …even if u need to write something which you’ve written earlier…you will have to open up the thesauraus and reframe your sentences…these are really usefull links…written by emminent personalities and also source of the above sentences….:D.[NTS] [BNS]
Actually thats what is happening… the so called “Researchers” used Salami Slicing and on top of that use Plagiarism and come up with even more articles….its actually a very tedious job…but hell!!! the results are rewarding..
Brings me to “RETRACTION WATCH”…Its kind of a “BIG BROTHER” ..here you can get all the news of who got screwed and for what and where and why….Google it please.
“The essential feature of pathological publishing is the persistent and recurrent publishing of confirmatory findings (Criterion A) combined with a callous disregard for null results (Criterion B) that produces a ‘good story’ (Criterion C), leading to marked distress in neo-Popperians (Criterion D) [Google it]”
Possible criteria for pathological publishing:
a) Having an excessive eagerness to show, disseminate, and advertise one’s articles. This is reflected in a compulsive behavior that consists of including one’s publications and indicators of one’s publications in numerous devices.
b) Falsifying articles including false or manipulated data in articles to obtain more publications or publish in journals with a higher impact factor.
c) Falsifying one’s CV including records of papers that are not such or duplicating articles.
d) Distorting reality believing the data that one has falsified or manipulated.
e) Distorting reality believing that something is an article when it is not (e.g., book reviews, meeting abstracts, editorial material, proceeding papers, notes).
f) Counting citations to one’s work and updating the number frequently.
g) Counting article downloads
h) Calculating the cumulated impact factor and updating it frequently.
i) Publishing anything to increase the number of publications
j) Continuously updating one’s CV
k) Including one’s CV and various indicators of the CV in a personal web page.
l) Including ResearcherID or other indicators in web pages that include the production of colleagues.
m) Using Web 2.0 to increase the number of citations.
Writing a blog is also considered in the above criteria..(OUCH!!)
Marketing of CV is actually considered a form of pathological publishing.
Now this can go on and on …..better read the article which also the source of inspiration for the above para….these guys have done a fantastic job….the direct link to it….
You know the productivity can be increased by showing more positiv results and tactfully excluding out the negative ones….actually it is more complicated than that but to simplify it …here is an example….
“An unavoidable confounding factor in this study is the quality and prestige of academic institutions, which is intrinsically linked to the productivity of their resident researchers. Indeed, official rankings of universities often include parameters measuring publication rates [39] (although the validity of such rankings is controversial [40], [41]). Therefore, it could be argued that the more productive states are also the ones hosting the “best” universities, which provide better academic structures (laboratories, libraries, etc…) and more advanced and stimulating intellectual environments. This could make scientists better at picking up the right hypotheses and more successful in testing them, increasing their chances to obtain true positive results. Separating this quality-of-institution effect from that of bias induced by pressures to publish is difficult, because the two factors are strictly linked: the best universities are also the most competitive, and thus presumably the ones where pressures to produce are highest.
A possibility that needs to be considered in all regression analyses is whether the cause-effect relationship could be reversed: could some states be more productive precisely because their researchers tend to do many cheap and non-explorative studies (i.e. many simple experiments that test relatively trivial hypotheses)? This appears unlikely, because it would contradict the observation that the most productive institutions are also the more prestigious, and therefore the ones where the most important research tends to be done.
What happened to the missing negative results? As explained in the Introduction, presumably they either went completely unpublished or were somehow turned into positive through selective reporting, post-hoc re-interpretation, and alteration of methods, analyses and data. The relative frequency of these behaviours remains to be established, but the simple non-publication of results is unlikely to be the only explanation. If it were, then we should have to assume that authors in the more productive states are even more productive than they appear, but wastefully do not publish many negative results they get.”
Furthermore, “Scientists/Researchers/Doctors” have known to cook up data..Ever wondered how certain people just keep on getting better and better results….certain studies are just too much in support of certain medications or machines or institute…[SOURCE]
Scientists also manipulate data to make their study look more positive…deliberate attempt to decrease the negative effects of a particular study by menitioning it less…and here the fellow/resident keeps on sratching his head wondering …”WHERE AM I GOING WRONG???THIS ISNT SUPPOSED TO HAPPEN”…[SOURCE]
On jre.sagepub.com, search for “Publication Pressure and Scientific Misconduct in Medical Scientists” by Joeri K. Tijdink, Reinout Verbeke, and Yvo M. Smulders.
IMPACT FOCTOR
[INTENTIONLLY]
“The impact factor (IF) is frequently used as an indicator of the importance of a journal to its field. It was first introduced by Eugene Garfield, the founder of the Institute for Scientific Information.[1] Although IF is widely used by institutions and clinicians, people have widespread misconception regarding the method for calculating the journal IF, its significance and how it can be utilized. The IF of a journal is not associated to the factors like quality of peer review process and quality of content of the journal, but is a measure that reflects the average number of citations to articles published in journals, books, thesis, project reports, newspapers, conference/seminar proceedings, documents published in internet, notes, and any other approved documents (by Indian Council of Medical Research or similar body).[2]
Impact factor is commonly used to evaluate the relative importance of a journal within its field and to measure the frequency with which the “average article” in a journal has been cited in a particular time period. Journal which publishes more review articles will get highest IFs. Journals with higher IFs believed to be more important than those with lower ones.[3] According to Eugene Garfield “impact simply reflects the ability of the journals and editors to attract the best paper available.”[4] Journal which publishes more review articles will get maximum IFs.
Impact factor can be calculated after completing the minimum of 3 years of publication; for that reason journal IF cannot be calculated for new journals. The journal with the highest IF is the one that published the most commonly cited articles over a 2-year period. The IF applies only to journals, not to individual articles or individual scientists unlike the “H-index.” The relative number of citations an individual article receives is better evaluated as “citation impact.” In a given year, the IF of a journal is the average number of citations received per article published in that journal during the 2 preceding years. IFs are calculated each year by Thomson scientific for those journals that it indexes, and are published in Journal Citation Reports (http://www.thomsonreuters.com/products_services/science/science_products/a-z/journal_citation_reports/). For example, if a journal has an IF of 3 in 2008, then its papers published in 2006 and 2007 received three citations each on average in 2008. The 2008 IFs are actually published in 2009; they cannot be calculated until all of the 2008 publications have been processed by the indexing agency (Thomson Reuters). The IF for the biomedical journals may range up to 5-8%.[5] The IF of any journal may be calculated by the formula;
2012 impactfactor =A/B
Where A is the number of times articles published in 2010 and 2011 were cited by indexed journals during 2012. B is the total number of citable items like articles and reviews published by that journal in 2010 and 2011.
The calculation of IF for the journal where in a person has published articles is a contentious issue. Nevertheless, this have been already warned; “misuse in evaluating individuals” because there is “a wide variation from article to article within a single journal” therefore, “In an ideal world, evaluators would read each article and make personal judgments,” said by Eugene Garfield.[1]” [SOURCE]
Now do you get why I wanted to discuss this the last??? Being a dynamic entity, its importance is hyped too much. You (the journal,editors, reviewers) can manipulate it the way they want to.
Just a hint..”Consequently some editors aimed at decreasing the number of published manuscripts, thereby selecting the higher priority articles leading ultimately to a higher earned JIF. Among citable articles, reviews are more commonly cited than original research papers[13] because reviews are authoritative, and are the synthesis of past multiple original research works of a topic in depth. This accounts for the fact that Progress in Retinal and Eye Research tops the list for JIF. Case reports are clearly of lesser academic value than original and review articles[14] and tend to lower JIF. Hence some editors (like Retina and American Journal of Ophthalmology) stopped publishing case reports. Basic science subjects like biochemistry, cell biology, and immunology have a very high JIF. Similarly, basic science journals in ophthalmology had high JIF with Investigative Ophthalmology and Visual Sciences ranking first over several years. Journals with high volume of original basic and clinical research and covering wide topics had high JIF, like Ophthalmology, Archives of Ophthalmology, American Journal of Ophthalmology, and British Journal of Ophthalmology.” [SOURCE]
Well….in this world where Doctors are writing books on “how to improve their private practice” and articles being submitted on “how to increase the visibility of your articles”…i guess these manipulations can also be taken in a stride.
Time and again people have pointed out the limitations of the “IMPACT FACTOR”….[Take a look] ..but we are back to square one everytime..last but not the least supporting evidence.
“The citation index of all journals is calculated from their citations alone. Crucial means of influencing the impact factor result from self-citations and citation groups in these source journals. Languages other than English and other than Latin alphabets are appreciably disadvantaged by the citation index, which is why for example despite its international significance the rapid development of the osteosynthesis technique in German speaking countries went unnoticed by British and American orthopedic surgeons and scientists. The articles on postgraduate training necessarily published by clinicians in the respective language of their country are not cited because the addresses of such publications do not engage in research. Clinical disciplines (especially highly specialized disciplines such as trauma and hand surgery) thus attain appreciably lower impact factors for their journals than basic disciplines and interdisciplinary clinical sectors which lead the ranking of journals. The period covered in calculating the impact factor is only 2 years. Very modern and widely disseminated organs of publication with a short information halflife are favored. From the 10 objectively most often cited and most important journals for the scientific society, only 2 are to be found amongst those with the highest impact factor. The impact front-runner from 1995 has a very low absolute number of citations. The impact factor provides limited statistical information on a journal in its special field. Using it for this purpose presupposes knowledge of rules, limitations and constraints. Its uncritical use as a general currency of science is fundamentally unscientific. In addition, this leads to the specialists in the field knowledge of the universities being disregarded in favor of a pseudo-objective parameter determined elsewhere. At all events, correction factors for the impact factor have to be applied in respect to the different disciplines. The faculties should reach agreement on relevant (also on German language) organs of publication. The impact factor is not suitable as an indicator of the research activity and the quality of a researcher or an institution. Besides careful human judgement and other classical methods of decision making, the Science Citation Index can contribute to the individual evaluation.” [SOURCE]
Right from the time immemorial hierarchy plays a major role in Medical field. Whatever the senior says is correct and whatever the senior does is correct.
Hence when a topic comes to the mind of a junior..naturally the first piece of pie will be eaten by the senior…the work is done by the junior, but the author will be senior.
So the Augmented layer is formed by the residents, The expected layer by the Assistant professors and fellows…whereas the product is devoured by the Boss!!!..Many times residents and fellows have their topics hijacked and used by seniors without their consent….most of the times these poor souls dont have the means to prove it but there are instances where the claim has been credited and the senior has been asked to retract the paper.
So all this is laid bare for you. Incase I have missed giving credit (discredit) to anyone, please feel free to write to me and i shall make the necessary changes. And still when someone asks me…”HOW MANY PAPERS HAVE YOU PUBLISHED??” ….my reply is ..” I AM NOT A JOURNALIST OR A WRITER….I AM A SURGEON…ASK ME HOW MANY CASES I HAVE OPERATED UPON…CAUSE NEXT TIME YOU WANT A SURGEON FOR YOUR MOTHER, YOU MIGHT WANNA CONSIDER ME!!”
After reading & writing all this one question is lingering in my mind….
WATCH THIS SPACE FOR DEVELOPMENTS…which I am sure is bound to happen…
Again…if i have missed out on mentioning anything or anyone, please feel free to write to me….my profile has my details…If you are calling to pick a fight….please dont….cause this is just a BLOG!!…noone takes it seriously..
Ask yourself these questions…even if one of them is being answered in affirmative by you please continue reading further….
1. Spending a short time or a moderately short time on the slit lamp and the operation theatre gives you a bad headache, Dizziness???Irritability???Nervousness??? Apprehension???
2.Did you have a tough time when you started operating or are having it right now??Are you not able to judge the position of the posterior capsule or get the inner lip of the section right??Do you often seem to have a bad complication when everything seems to be going right ??
3.Having a really steep learning curve when it comes to surgery??
4.You seem to be doing everything correctly but still things don’t work out, the trainer has long since given up on you…
5. The indirect ophthalmoscope and you don’t get along very well. Have you wondered why you’ve taken so long to master IO?? or you might still be struggling. Learning the “ART” of IO is a tough one and requires a lot of practice…..but there is one factor which we keep on ignoring often….keep on reading….
6.You, yourself are unable to use the 3D glasses, have a headache while using one. Even though a particular 3D movie was a big hit you didn’t really enjoy the special effects. More often patients come complaining about a headache which they developed after entering a cinema hall and it persisted through out the movie. The headache disappeared after this particular person rested for sometime.
You get up in the morning, have a hearty breakfast, enter the OPD in high spirits or the operation theater for that matter…you feel you are an excellent clinician and a damn good surgeon….Oops….JINXED…right in the middle of your 2nd case you land into trouble.
Many people attribute the above mentioned problems to a variety of causative factors. Your trainer tells you that you don’t have it in you to be a surgeon. Your guide says that you are not paying attention. The instrument is fine, its you who is faulty. You are a slow learner….you were not meant for this field…you are not following the directions properly…The headaches are termed as tension headaches and the cause of tension is you yourself.
The age old ritual of learning the “HAND EYE CO-ORDINATION” for an ophthalmologist is something we all go through during our residency. But there are some of us who have a tough time …
Many of you are being coached by “LITERATE” seniors who tell you that …”It’s ok…you are getting used to the slit lamp….and your hand eye co – ordinationwill develop soon’…
But in reality many of us keep on using our eyes in an un co-ordinated fashion and usually without even realising it keep one eye in a suppressed mode…Now we all have learnt that the depth preception comes when the binocular vision is intact.
SO….if you have one eye in the suppressed mode and the other eye is used for developing the hand eye co-ordination …HOW THE HELL are you gonna get things straight..???
Before you guys jump to any conclusion….suppression can be a temporary thing…so think about it….you using the slit lamp and the 90 D lens seems funny …..The indirect ophthalmoscopy we are unable to judge the depth while a colleague is nicely basking in the glory of the seniors in being able to see those damn vitreous floaters….
What exactly is this entity and how significant is the problem??
This is just the tip of the iceberg….Patwardhan SD, Sharma P, Saxena R, Khanduja SK. Preferred clinical practice in convergence insufficiency in India: A survey. Indian J Ophthalmol [serial online] 2008 [cited 2016 Jul 24];56:303-6. Available from: http://www.ijo.in/text.asp?2008/56/4/303/39661…34% ophthalmologists claimed >10% patients in the outpatient department (OPD) with CI requiring treatment, while 22.7% ophthalmologists suggested that they attend to 6-10% OPD patients with CI.
A pilot study done by me revealed that the incidence might be closer to approximately 72% in Indian population and closer to 55% in the Ophthalmologists.(UNPUBLISHED OFCOURSE!!!)
The “CONVERGENCE INSUFFICIENCY SYMPTOM SURVEY” is something you should go through…but it doesnt help much except tell you what you already know deep down….you are having a problem with your eyes and the SLIT LAMP AND THE OPERATING MICROSCOPES are your worst enemies (Ignoring the ignorant, learned people here)
Now….many people seem to have a normal Near point of convergence…..but its the fusional capacity which is defective….although the majority cases seem to have convergence insufficiency and fusional insufficiency going hand in hand.
Now back to basics…WE ALL KNOW…that phoria for near means convergence insufficiency….but guys ….AS “ROLAND” from the famous novel series (The dark tower) by Stephen King says…
“THE WORLD HAS MOVED ON”…
As a resident in majority of the institutes across India we have been refrained from learning about the beautiful art of refraction. There is a new breed of Clinicians who are called as
“VISION THERAPISTS”. these guys actually know their stuff…for that matter our stuff…
WE as residents and ophthalmologists are taught about refraction and after reading those exhaustive books, a pseudo sense of knowledge is instilled in our minds…Giving a prescription for hypertropia is the peak of that knowledge and we consider ourselves “LEARNED”.
The World has really progressed….the vision is not something we remember studying as form sense, colour sense and all that…It goes beyond that…
Enough of the gyan…coming back to the topic…Phoria for near is basically convergence insufficiency for us …but now those things have been sub divided.
Let me put it this way….you have trouble while reading or operating…or any of the following things…(From the immensly talented Dr KHURANA’s text)…go on …read it to the last point…you might be suffering from some of this…
Tired, aching, Bleary eyes.
Dull aching, Boring, superficial, deep seated & migranous kind of headache.
A general headache
Frontal, temporal, vertical, occipital headache
Tender vertex or temple.
Sharp shooting and lancinating pain.
Intermittent blur
Itermittent diplopia
Symptoms worse at the end of the day or end of an OT session
Inability to concentrate or sustain
Words move or swarm.
Slow reading
Digestive upsets….yes…you are reading it correctly.
Dyspepsia
Nausea
Vague nervous disorders
Insomnia
DEPRESSION
Apart from this the list goes on and on ….and on…. there are many such problems plaquing us. Last but not the least, you have a dysfunction and then teary eyed…and then the constant rubbing….aggravating the already existing allergic conjunctivitis (which btw is almost universal now). Kid coming to you ..or and adult coming to you with non responsive or suboptimally responsive allergic conjunctivits…pray do check his fusion.
Yet again…coming back to the topic…these asthenopic symptoms can be due to convergence insufficiency or due to fusional vergence dysfunction or rarely due to divergence excess.
Now the convergence insufficiency can be tackled by the simple pencil push ups prescribed by the ” LEARNED SENIORS” …but in reality we are touching only the tip of the iceberg.
The FUSIONAL VERGENCE DYSFUNCTION is an equally notorious entity.
There have been quite a lot of studies which have tried to co relate the symptoms versus the signs for convergence insufficiency and have failed to do so. Thats because the above factors have not been considered. Hopfuly with the developing knowledge people will come up with studies.
We have tests such as the vision balance and the muscle balance, where the positive and negative fusion capacities are measured. But are we measuring what is truly required…infact…are we measuring what is really theoretically and practically correct??? “HALF KNOWLEDGE IS DANGEROUS” ..it holds very true here….Giving a patient or yourself a simple pencil pushups is not going to help ….the problem doesnt end there.
Go on…go back and open your books…you wont find the above mentioned term there….you need to get in touch with the books which mention about these things..wondering where you’ll get those…get in touch with me…ill show you the way.
A simple pencil pushups are not going to help you….you need to really get a professional help. Do you know what this is ??
Probably you dont…if you do then ive wasted your time…and if you dont…then this is a BROCK STRING…uses and benefits…GOOGLE it…
Also what the hell is “NONSTRABISMIC BINOCULAR VISION DISORDER”. You are probably scratching your head and wondering what the hell is this….if not then good for you.
There are many things which we are not allowed to learn in our residency… and i am being clear…”NOT ALLOWED”. A simple vision assessment and prescription of glasses is not enough.
We have used the dot card which is good but do you know where to get it from?? how to create your own dot card?? How to really use it properly??
Ahh….forgot….almost…the 3D glasses….Fusion disorders are the answer.
This problem is not limited only to our group of ophthalmologists. The list goes beyond that. The students, IT Professionals…..
Simply waiting for the hand eye co-ordination to develop and getting “USED” to the slit lamp is not gonna help.
This blog is simply to create awareness and not to provide you with a text which you can read and go on to practice…make some effort…find a professional and get urself treated.
Thank you for reading and please contribut by leaving comments. If i have failed to mention anyone please feel free to contact me and i shall rectify. Watch this space for developments. Follow if you wanna know whats cooking!!
BTW my last blog has almost reached to 5000 professionals…HURRAY!!!
When you are aspiring to be an ophthalmologist, little do you know that around 50% of the existing opthalomologists suffer from some form of MSD (Musculoskeletal disorder).
So what makes us so prone to these disorders???
It’s the lack of knowledge and the lack of self-regard. We are so much immersed in the well-being of the patient that we forget to stop and think about ourselves. Unfortunately this in the long run, or for some like me, in a short duration spells doom.
I used to be a high volume surgeon and spend 8 – 9 hours every day operating on 60 – 70 patients in a day. The Opd was the next stop, which meant another 80 – 100 patients. The pains followed soon, within 3 years into my professional life.









 (Like peeing in the basin or venturing out of the washroom without your shorts) after a long day of work at the professional front indicate the wearing off the sympathetic system activity. This often forces many of us to choose between the two, the professional or the domestic life. Striking a balance becomes difficult for many of us.
(Like peeing in the basin or venturing out of the washroom without your shorts) after a long day of work at the professional front indicate the wearing off the sympathetic system activity. This often forces many of us to choose between the two, the professional or the domestic life. Striking a balance becomes difficult for many of us.



 grandfather), you pay the journal to publish it and then the journal gets paid for others to read.
grandfather), you pay the journal to publish it and then the journal gets paid for others to read. some facts..Pubmed on an average has 1.4 million to
some facts..Pubmed on an average has 1.4 million to
 west for money..came to the east and the rest of the world as the Number game. People are just running after numbers not knowing the goal. The only goal achieved here in the east is “FAME“. The western counterparts earn money and the eastern counterparts earn Fame. Whatever is published there (in west i mean) is science and native journals are crap. So we are all running in the rat race to publish in the western journals.
west for money..came to the east and the rest of the world as the Number game. People are just running after numbers not knowing the goal. The only goal achieved here in the east is “FAME“. The western counterparts earn money and the eastern counterparts earn Fame. Whatever is published there (in west i mean) is science and native journals are crap. So we are all running in the rat race to publish in the western journals.
 patients. They,ve got the knowledge but unable to replicate on the paper. Some of these people are damn good clinicians and surgeons, but due to inability to “PUBLISH” or “ADVERTISE (how i see it)”, remain unknown to the majority of the opthalmological community. Though their patients are really happy and are well known in the community.
patients. They,ve got the knowledge but unable to replicate on the paper. Some of these people are damn good clinicians and surgeons, but due to inability to “PUBLISH” or “ADVERTISE (how i see it)”, remain unknown to the majority of the opthalmological community. Though their patients are really happy and are well known in the community. data and publishing it. They are usually co-authors in a number of studies though they dont have anything to do with the actual thing. They may be good clinicians or surgeons, but the lack of reproducing the data on paper is compensated by being a part of other’s.
data and publishing it. They are usually co-authors in a number of studies though they dont have anything to do with the actual thing. They may be good clinicians or surgeons, but the lack of reproducing the data on paper is compensated by being a part of other’s. who dont have good knowledge or publishing capacity and are just scrapping through. They train themselves in doing the most basic of things in ophthalmolgy and keep on surviving in this competitive world.
who dont have good knowledge or publishing capacity and are just scrapping through. They train themselves in doing the most basic of things in ophthalmolgy and keep on surviving in this competitive world. conferences (R U KIDDING ME!!)…
conferences (R U KIDDING ME!!)… . Not all are gifted with the calibre to write….and not all gifted with the calibre to operate….Put Sachin Tendulkar in the kitchen and you will have a disaster. Intelligence quotient is relative.
. Not all are gifted with the calibre to write….and not all gifted with the calibre to operate….Put Sachin Tendulkar in the kitchen and you will have a disaster. Intelligence quotient is relative. number of publications for promotion in the teaching line is just ridiculous…A good teacher might not be a good researcher….and vice versa…but unfortunately the propaganda has been too strong..This often lead to the seniors hijacking the topics of the residents or setting up deadly deals with the residents (NO TOPIC, NO HOLIDAYS).
number of publications for promotion in the teaching line is just ridiculous…A good teacher might not be a good researcher….and vice versa…but unfortunately the propaganda has been too strong..This often lead to the seniors hijacking the topics of the residents or setting up deadly deals with the residents (NO TOPIC, NO HOLIDAYS).
 paper goes through the journal editorial board (usually a computer)…they send it out to scientists (working and hard working personnels themselves!!) …these guys read the whole thing (Guessing that they read, there are softwares to generate reviews)…understand/misunderstand/not understand/confuse the concept and then the review is given which is directed back to you. Now either you are rejected immediately or after making a number of corrections/alterations. This process can be blinded or not…What I mean is that the journal can select which persons should recieve your article or you can select on your own.
paper goes through the journal editorial board (usually a computer)…they send it out to scientists (working and hard working personnels themselves!!) …these guys read the whole thing (Guessing that they read, there are softwares to generate reviews)…understand/misunderstand/not understand/confuse the concept and then the review is given which is directed back to you. Now either you are rejected immediately or after making a number of corrections/alterations. This process can be blinded or not…What I mean is that the journal can select which persons should recieve your article or you can select on your own. humans…These reviewers are supposed to be “GATEKEEPERS” for the protection of the science, but most of them are practicing doctors and researchers…they have their own methods, interests, conflicts, pressures. A study submitted to a reviewer who might be working on a similar project will force the person to reject it. A single person serving on the review board of 20 journals, receiving 150 articles in a month, operating and attending to his patients is bound to make a mistake or miss something.
humans…These reviewers are supposed to be “GATEKEEPERS” for the protection of the science, but most of them are practicing doctors and researchers…they have their own methods, interests, conflicts, pressures. A study submitted to a reviewer who might be working on a similar project will force the person to reject it. A single person serving on the review board of 20 journals, receiving 150 articles in a month, operating and attending to his patients is bound to make a mistake or miss something.
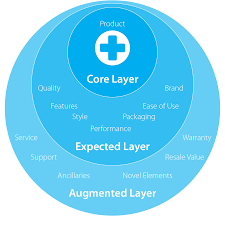

 though a particular 3D movie was a big hit you didn’t really enjoy the special effects. More often patients come complaining about a headache which they developed after entering a cinema hall and it persisted through out the movie. The headache disappeared after this particular person rested for sometime.
though a particular 3D movie was a big hit you didn’t really enjoy the special effects. More often patients come complaining about a headache which they developed after entering a cinema hall and it persisted through out the movie. The headache disappeared after this particular person rested for sometime. something we all go through during our residency. But there are some of us who have a tough time …
something we all go through during our residency. But there are some of us who have a tough time …
 University Students”,Optometry & Vision Science:
University Students”,Optometry & Vision Science:
 learning about the beautiful art of refraction. There is a new breed of Clinicians who are called as
learning about the beautiful art of refraction. There is a new breed of Clinicians who are called as